Deep Support, Gravity Considerations & the Role of SMAS-Level Placement The safety, longevity, and aesthetic outcome of dermal filler treatment depend heavily on the anatomical plane of injection. This article reviews the rationale for deep versus superficial placement, evaluates whether fillers placed in unsupported soft tissue contribute to sagging over time, and clarifies whether sub-SMAS …
Deep Support, Gravity Considerations & the Role of SMAS-Level Placement
The safety, longevity, and aesthetic outcome of dermal filler treatment depend heavily on the anatomical plane of injection. This article reviews the rationale for deep versus superficial placement, evaluates whether fillers placed in unsupported soft tissue contribute to sagging over time, and clarifies whether sub-SMAS injection provides meaningful mechanical lift.
Introduction
Modern facial rejuvenation has shifted from line-based filling to structural, anatomically guided volumisation. Correct plane selection is now central to avoiding complications, preventing heaviness, and generating predictable lift.
Do Fillers “Drop” When Injected Into Unsupported Tissue?
2.1 Not true descent from gravity — but soft-tissue biomechanics matter.
Hyaluronic acid fillers are cohesive gels that do not migrate downward due to gravity.
However, in mobile soft tissue compartments lacking osteocutaneous ligament support, injected fillers may:
- Displace with repeated facial expression (dynamic shear)
- Spread superficially over time
- Increase soft-tissue mass in regions already prone to age-related descent
- Contribute to mid-face heaviness or a pseudo-ptotic appearance
This phenomenon is often misinterpreted as “filler drooping,” but it is better described as soft-tissue overloading.
2.2 Why deeper injections prevent heaviness
Deep compartments, periosteum, and ligamentous origins are low-mobility, high-resistance environments, allowing filler to:
- Maintain its projection
- Provide vertical support
- Require lower total volumes
- Avoid adding weight to gravitationally vulnerable tissues (e.g., the lower cheek)
Multiple cadaveric studies confirm that deep facial fat pads are more stable with minimal shear forces, supporting deep injection as the preferred method.
Deep Structural Volumisation (Bone-Level)
Injection on or just above the periosteum (supraperiosteal plane) remains the most structurally efficient technique for:
- Malar projection
- Zygomatic anchoring
- Chin and prejowl correction
- Jawline definition
- Temple reconstruction
Rationale
Bone-level placement reproduces the native bony foundation lost during ageing. Products placed here exhibit:
- Improved longevity
- Minimal lateral spread
- Strong vector support
- Lower risk of edema due to reduced vascularity

Ligament-Based Rejuvenation
The face contains key retaining ligaments (e.g., zygomatic, orbital, masseteric, mandibular ligaments) that can act as anchor points.
Injecting adjacent to ligament origins:
- Restores tension
- Improves vector lift
- Allows smaller volumes
- Enhances stability
- Reduces the need for superficial correction
This is a foundational principle of MD Codes®, BeautiPHIcation™, and the Ligament-Based Approach.
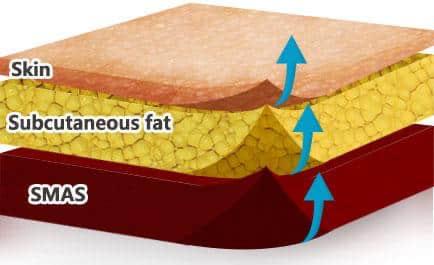
Should Filler Be Injected Under the SMAS for Maximum Lift?
Short answer: No — true sub-SMAS injection is not standard practice for fillers.
Reasons:
- The sub-SMAS plane contains motor branches of the facial nerve, making injection unsafe.
- In many regions, direct access to sub-SMAS levels is not possible without surgical dissection.
- Structural deep compartments (deep fat pads and periosteum) already provide the mechanical lift needed.
What practitioners mean by “deep filler under SMAS”:
They typically refer to:
- Deep medial cheek fat (DMCF)
- Lateral sub-orbicularis oculi fat (SOOF)
- Supraperiosteal plane
- Prezygomatic space
These planes lie beneath SMAS-associated structures and functionally behave like “SMAS-deep planes,” without requiring literal sub-SMAS injection.

Conclusion
The best lift from filler comes from deep, structural planes, not from sub-SMAS injection.
Summary — Evidence-Based Best Practices
Prefer deep injection when possible:
- Periosteum
- Deep fat compartments
- Ligament origins
Avoid heavy superficial filling in unsupported tissue:
- Malar “apple” area
- Lower cheek
- Lateral buccal space
Deep > superficial for:
- Longevity
- Stability
- Lift
- Natural contour
- Reduced edema and heaviness
Superficial injections remain necessary for:
- Fine lines
- Tear trough blending (with caution)
- Skin quality improvement (skinboosters)
Peer-Reviewed References
Filler biomechanics, movement, and support planes
- Gierloff M, Stöhring C, Buder T, Wiltfang J, Gassling V. Aging Changes of the Midfacial Fat Compartments: A Computed Tomography Study. Plast Reconstr Surg. 2012.
- Rohrich RJ, Arbique GM. The Anatomy of Facial Aging: A 3-Dimensional Perspective. Plast Reconstr Surg. 2016.
- Mendelson BC, Wong CH. Changes in the Facial Skeleton With Aging: Implications for Facial Rejuvenation. Aesthet Surg J. 2012.
Deep versus superficial injection outcomes
- DeLorenzi C. Complications of Injectable Fillers, Part I. Aesthet Surg J. 2013.
- Beleznay K, Humphrey S, Carruthers JD. Migration of Injected Fillers. Dermatol Surg. 2015.
- Rzany B, Griffiths T. Supraperiosteal Filler Injection Techniques for Structural Support. J Cosmet Dermatol. 2019.
Ligament-based injection principles
- Furnas DW. The Retaining Ligaments of the Face. Plast Reconstr Surg. 2015.
- Wong CH, Hsieh MK. Facial Ligaments and Their Clinical Application. J Plast Reconstr Aesthet Surg. 2015.
- Mendelson BC. Understanding the Facial Ligamentous System. Plast Reconstr Surg. 2011.
SMAS and deep filler placement
- Mowlavi A, Massry GG. Sub-SMAS Anatomy Relevant to Injectables. Aesthet Surg J. 2018.
- Wan D, Chen J. Deep Fat Compartments and Their Role in Filler Placement. Aesthetic Plast Surg. 2020.
- Cotofana S, Schenck TL. The Anatomy of the SMAS and Its Implications in Minimally Invasive Procedures. Clin Anat. 2021.
Filler mechanics, rheology, and tissue behavior
- Sundaram H, Cassuto D. Biophysical Characteristics of Hyaluronic Acid Fillers. Dermatol Surg. 2013.
- Gold MH, Sadick N. Rheology of HA Fillers and Clinical Relevance. J Clin Aesthet Dermatol. 2018.
- Liew S, Wu WTL. Facial Shape and Biomechanics in Filler Injection. Dermatol Surg. 2020.
Book a Consultation
It’s easy and free!